
Your Pregnancy Help Organization and COVID-19
If you are a Heartbeat Affiliate, please click log in at the top of the page to view more materials! Additional materials will appear below for those current affiliates who are already logged in. Click here for more information about affiliating with Heartbeat International.
You can also get a recording of our webinar series Coronavirus and Your Pregnancy Help Organization for free by clicking here. Resources related to those webinars are also available on the Complimentary Materials page here.
The information in these articles is accurate as of the publication date of each one. We are working to keep our articles up-to-date as changes surrounding COVID-19 occur, and we encourage everyone to check the CDC, WHO and their local authorities as the situation is ever-evolving.
Displaying items by tag: ultrasound
Transvaginal Sonogram: Is it Necessary in Your Medical Center?
by Audrey Stout, RN, RDMS, SoundView Imaging Partners
 |
In over ten years of educating abortion-vulnerable women on fetal development and abortion, I had seen many of these women experience a change of heart. Yet, for years, I also believed that if a woman was able to see her unborn child through ultrasound, many more would choose life. From the very beginning, we knew transvaginal ultrasound to be the best means of imaging a pregnancy in the early stages.
One objection we may not have anticipated was this: “We don’t want to do that, do we? What if the girls have not had a bath before coming?” Our medical team appropriately determined that we must “do that,” and then learned to perform both abdominal and transvaginal ultrasounds in order to provide pregnant women with services equal to the standard of care in the broader medical community.
Even with more than 600 pregnancy medical clinics offering medically indicated limited OB ultrasounds, there is still a lack of a common understanding for the necessity of transvaginal ultrasound in the pregnancy medical clinics, which bears itself out in resistance or hesitance to utilize this valuable resource. But transvaginal sonograms are absolutely necessary for pregnancy medical clinics.
The Importance of Transvaginal Ultrasound
For early pregnancies, as well as women with a retroverted uterus or obesity, the use of transvaginal sonography is critical to determine the location of the pregnancy, since the child is tiny, and often not visible when scanning abdominally.
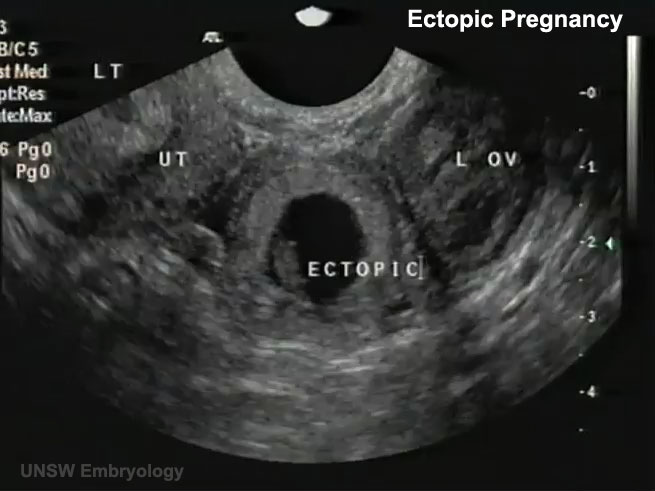
During a recent training involving around 60 scans, there were two patients for whom it was impossible to determine if there was a true gestational sac or pseudo sac of an ectopic pregnancy in the uterus by scanning abdominally. When the transvaginal probe was used, however, both ultrasounds revealed tiny embryos with beating hearts, measuring from 2-3 mm (25 mm=1 inch) in length alongside a yolk sac—diagnostic for an intrauterine pregnancy.
Apart from using the transvaginal probe in each of these cases, the patients would have needed both ectopic and miscarriage precautions, due to an inconclusive ultrasound. This would have required a follow-up scan, either at the PMC or with another physician, for serial hCG levels, in addition to another sonogram to rule out an ectopic pregnancy. This would have caused needless stress and concern, when the answers were available with a transvaginal scan. When a woman seriously considering abortion comes into a pregnancy clinic, we may only have one opportunity to see her and provide a life-affirming sonogram.
The three medical indications, for performing a limited OB sonogram in most PMCs according to the American Institution for Ultrasound in Medicine:
- To confirm the presence of an intrauterine pregnancy.
- To confirm cardiac activity.
- To estimate gestational age (EGA).
From the Textbook to the Pregnancy Medical Center
Every woman considering abortion needs this information to make a truly informed choice regarding her pregnancy. Using transvaginal sonography during the first trimester, one is much more likely to be able to answer the three questions listed above, and enable a woman to see the life of her unborn child in order to refute the idea that her child is just a mass of tissue.
PMCs typically see women in early pregnancy when they are most likely to have ectopic pregnancies, as most show symptoms between 7-8 weeks LMP. Since a ruptured ectopic pregnancy is life-threatening due to massive hemorrhage, every early sonogram must attempt to determine the location of the pregnancy. Ectopic pregnancy is the leading cause of first trimester maternal death, even though less than 9% of ectopics are actually visualized with a fetal pole on sonography because they are notoriously difficult to diagnose.
Skill in both transabdominal scanning and transvaginal scanning are necessary, as some ectopics or associated findings are visible with abdominal scanning, while most can only be visualized using transvaginal scanning. Transvaginal sonography also can uncover a rare condition known as “heterotopic pregnancy,” which is both intrauterine and ectopic, occurring at a rate of 1/30,000 in natural reproduction.
A recent article from MedPage Today discusses ectopic pregnancies and highlights the need for using transvaginal sonography. The article states:
Ectopic pregnancy occurs in up to 2.6% of all pregnancies and is the chief cause of first-trimester pregnancy-related mortality, accounting for up to 6% of maternal deaths. However, less than half of women with ectopic pregnancy have characteristic symptoms of abdominal pain and vaginal bleeding, which are more likely to indicate miscarriage.i
Further, ectopic pregnancy has been on the increase since 1970, when the Center for Disease Control began tracking this condition.
Key Factors to Keep in Mind
As those performing ultrasound services in the PMCs, adequate training is critical in order to gain skills in imaging the maternal anatomy, demonstrating with every sonogram that the pregnancy is intrauterine (IUP). If one does not possess these skills, it puts not only the woman who comes to you at-risk for losing her life, it also puts your PMC at legal risk of liability for harm. Thankfully, many women have been protected from life-threatening ectopic ruptures, due to the careful and skillful scanning of nurses and other medical personnel in PMCs.
Here are five tips to protect all involved by safely performing sonograms to the highest standard of medical care in your PMC:
- Attend a foundational didactic course for performing Limited OB Sonography in accordance to the Association of Women's Health, Obstetric and Neonatal Nurses Guidelines (AWHONN), e.g. the NIFLA course (NIFLA.org).
- Gain adequate hands-on training by an RDMS or physician skilled in performing OB sonograms to demonstrate competency in skills, both abdominally and transvaginally before performing sonograms without direct supervision. A minimum of 50 scans is strongly recommended for every sonographer, though for most, 60-75 may be needed. Documented competency is key to safety in scanning. Those skills should be assessed and refreshed on an annual basis.
- Follow a systematic scanning protocol, always beginning with an abdominal survey of the pelvis (including the adnexae and uterus) in two planes to identify the pregnancy location and get an idea of the gestational age.
- If with abdominal scan, one cannot clearly visualize anatomy (the vagina, cervix and contents of the uterus, i.e. gestational sac and fetal pole) with a high level of resolution to demonstrate an IUP, perform a transvaginal scan throughout the first trimester. When an IUP is not demonstrated, one must always suspect ectopic and provide precautions. Never assume it is too early.ii
- Consider sonography a life-long learning and skill journey, with excellence as the goal. For competency and skills growth, a sonographer should perform approximately 100-150 scans each year.
So, are transvaginal sonograms necessary in your PMC? Yes, yes, and yes.
Transvaginal sonograms safely provide sonography services and protect those served. In fact, sonographers with adequate training often happily admit, once they have acquired the skills, they very much prefer transvaginal scans because of the superior resolution and the fact that women are able to clearly see the image of their unborn child.
________________________________________
Audrey Stout, RN, RDMS, has a passion for the cause of life and began involvement with pregnancy centers in 1987. In 2000, she began instructing with NIFLA’s Limited OB Ultrasound Course and serves as National Nurse Manager Consultant for NIFLA as well. She has provided hands on trainings in sonography for PMCs medical personnel throughout the US, and is a founding partner with SoundView Imaging (SoundViewImaging.org). Audrey lives in Lexington, VA with her husband, Dave. They have three grown adopted children and one grandson.
Notes
i. Boyles, S. Transvaginal Ultrasound Best to Find Ectopic Pregnancy. April 23, 2013. Medpage Today. Accessed June 25, 2013 from: http://www.medpagetoday.com/OBGYN/Pregnancy/38638.
ii. Bourgon, D., Lin, E., Ectopic Pregnancy Imaging. April 12, 2011. Medscape. Accessed June 28, 2013 from: http://emedicine.medscape.com/article/403062-overview.
Pro-Life Prenatal Diagnostics
 Prenatal diagnosis is now much easier and safer than ever before. But, these advances also exist within a mix of conflicting and sometimes hidden agendas. January is Birth Defects Prevention Month, so there's no better time to examine the topic and focus on the critical role PHC/PMC’s play in preventing birth defects.
Prenatal diagnosis is now much easier and safer than ever before. But, these advances also exist within a mix of conflicting and sometimes hidden agendas. January is Birth Defects Prevention Month, so there's no better time to examine the topic and focus on the critical role PHC/PMC’s play in preventing birth defects.
The education we provide to our clients may be the determining factor in preventing a child from being born with birth defects, but this fact raises a great dichotomy to the surface: On one hand, we desire all mothers and babies to be healthy, and we should proactively educate them on how to achieve this. On the other hand, however, we must carefully construct our instruction in a way that avoids negatively influencing a client to seek an abortion if she should learn of a negative diagnosis regarding her baby.
Fetal problems are a serious rationale for considering abortion in our current culture, spurred in part by diagnosis of these abnormalities with the increased use of ultrasound, amniocentesis, and other tests in pregnancy. Ultrasound studies to determine fetal anatomy are often done at 18-20 weeks, so abortions done as a result of these scans are late abortions. But ultrasound is imperfect and analysis of the images can result in inaccurate interpretations.
Pregnant women who have declined abortion for fetuses diagnosed by ultrasound with fatal birth defects have sometimes ended up giving birth to normal babies. Other parents have resisted recommended abortions for serious anatomical problems, and had their babies undergo surgical repair after birth.
A great example of this truth comes from, Is Late-Term Abortion Ever Necessary?, an article by Mary Davenport, M.D., published on the American Association of Pro-life Obstetricians and Gynecologists website:
C. Everett Koop, M.D., the former surgeon general and renowned pediatric surgeon, was asked during the partial-birth abortion hearings if he had treated children “born with organs outside of their bodies” (omphalocele). Dr. Koop replied, “Oh, yes indeed. I’ve done that many times. The prognosis usually is good….the first child I ever did, with a huge omphalocele much bigger than her head, went on to develop well and become the head nurse in my intensive care unit many years later.”
For fatal birth defects, abortion is sometimes presented as the only option. But a better alternative is perinatal hospice. This involves continuing the pregnancy until labor begins and giving birth normally, in a setting of comfort and support until natural death occurs. It is similar to what is done for families with terminally ill children and adults. Karen Santorum, a nurse and the wife of former Senator Rick Santorum, was faced with the prospect of her own son, Gabriel, being born with a fatal birth defect. She describes how Gabriel lived only two hours, but how in those two hours “we experienced a lifetime of emotions. Love, sorrow, regret, joy—-all were packed into that brief span. To have rejected that experience would have been to reject life itself.” The sense of peace and closure felt by families experiencing neonatal death in a hospice setting contrasts markedly with the experience of families undergoing abortion for fetal anomalies. Couples who have had abortions for birth defects may suffer from adverse long-term psychological effects and prolonged grief reactions. Children who learn that their mothers aborted their siblings can suffer feelings of worthlessness, guilt, distrust and rage.
Non-fatal birth defects can be more challenging. The most common prenatal diagnosis resulting in mid-trimester abortion is Down syndrome. There has been an aggressive campaign by the American College of Obstetrics and Gynecology to use new technologies to detect Down syndrome in younger women through measurement of fetal neck-fold thickness and first trimester blood tests, now that prenatal diagnosis and abortion have succeeded in eliminating 90 percent of Down babies in women over 35. After diagnosis of Down syndrome, families are often not presented with an honest discussion of parenting their Down syndrome child, or the possibility of their Down syndrome child attending school and leading a semi-independent life. There are couples who are willing to adopt children with Down syndrome or other birth defects, but genetic counselors frequently do not give patients this information. Diagnosis of a child with a fetal anomaly is life-changing and a major stress, but many families rise to the occasion and are able to cope with a disabled child. Although parents choosing abortion may allege that the disabled child is better off not existing, disabled adults would contest that assertion. When surveyed in numerous studies, no differences have been found between disabled and “able-bodied” people as to their satisfaction with life.
A sad depiction of the haste to abort children with birth defects is captured in the following story, from LifeSiteNews.com:
GIA LAI PROVINCE, VIETNAM (May 16, 2012) --- A family is in grief after aborting a child erroneously reported to have congenital defects. The child died shortly after being born following a failed abortion. The mother, Nguyen Thi Thu T., had undergone two ultrasounds that falsely reported birth defects – one in her native Chu Se District and another in Ho Chi Minh City. She chose to abort the baby in the seventh month of her pregnancy. However, as the family gathered to bury the child, they found the baby was still alive and had no such defects. Although they rushed the child to Gia Lai Province General Hospital at 9:30 Sunday morning, it was too late.”
 Dr. Gerard Nadal offers some hopeful encouragement to this discussion. He says that, while some are fearful that the newer diagnostic tests for Down syndrome will lead to a higher number of abortions, the already-staggering number of 90-93 percent of unborn Down syndrome babies being aborted can also offer a glimmer of hope.
Dr. Gerard Nadal offers some hopeful encouragement to this discussion. He says that, while some are fearful that the newer diagnostic tests for Down syndrome will lead to a higher number of abortions, the already-staggering number of 90-93 percent of unborn Down syndrome babies being aborted can also offer a glimmer of hope.
The regrettably high number of Down syndrome babies being aborted means "there is not much room for (those numbers) skyrocketing", Dr. Nadal points out, and the advances in amniocentesis, which can diagnose Down syndrome as early as the 10th week, may actually offer parents more time to come to terms with the diagnosis and seek alternative advice earlier in the pregnancy than previously available.
Helping the parents come to terms with the reality of their child’s special needs ahead of time is critical for bonding. As those called to serve these parents, it is essential for pregnancy help medical personnel and peer counselors to understand just how devastating a negative diagnosis can be, so that we can provide help during a difficult time. The earlier the diagnosis, the more time we have to help them.
Still, there is a disturbing eugenic flavor to the fact that the American College of Obstetricians and Gynecologists (ACOG) and other groups are now recommending Down syndrome screening to all pregnant women. Many physicians are beginning to recommend that clients undergo non-invasive prenatal screening for fetal abnormalities, with a particular emphasis on Down syndrome.
As Steve Calvin, M.D., said in an article posted at AAPLOG.org January 11, 2007, “Women are reporting both subtle and overt pressure to undergo prenatal screening and to have an abortion if DS is found.”
This problem is further seen in the fact that most genetic conditions can be identified in the womb—including Down syndrome—yet, there are no available cures or therapies that can be administered before the child is born. Thus, a predominant purpose of prenatal screening is to offer parents the option of aborting “defective” babies. An estimated 70 percent of pregnant U.S. women will choose to have prenatal screening tests. A certain combination of screening results, though not definitive, can predict DS with up to 90 percent sensitivity.
Let us remind ourselves of the dignity and value of every person, who are all made in the image and likeness of God. Remember too that perfect health and a normal IQ are not required for happiness, friendship, and love of life. Rather than offering parents ways to eliminate their unborn child, we can provide them with more resources and support.
In her article found at PhysiciansForLife.org, Down Syndrome and Abortion, Susan W. Enouen, PE, wrote:
A Harvard study found that mothers who chose to continue their pregnancy after a prenatal diagnosis of Down syndrome did so for personal reasons such as conscience and religion, but also because they had gotten information about Down syndrome, either in printed materials or from talking to a parent of a child with DS. However, most of the mothers felt that their doctors did not explain DS adequately and in a balanced fashion.
This is where we can have a dramatic impact with a client who is facing a negative diagnosis. Let us become knowledgeable about the issues, develop resources for the client and extend to her the love, compassion, and prayerful support she so desperately needs.
International effects of ultrasound
By Connie Ambrecht RDMS, CMB
|
Heartbeat International has a heart for international ministry. If you would like to join in the international ultrasound ministry, there are a couple of resources of which you should be aware:
|
Have you wondered how much impact ultrasound could have internationally? What does it take? Who is qualified to go? Who would you train in those countries?
It almost sounds glamorous to travel to exotic places like Haiti and Ecuador or Ukraine and Romania. Hope Imaging and its teams have been to all of these countries and more, taking life-affirming sonography training to physicians, midwives, and nurses in these foreign lands.
If traveling internationally to address life issues doesn’t interest you, read no further. Hope Imaging is all about the God possibilities, and exotic travel and intrigue are all part of His itinerary to get the job done well.
You may already be interested and eagerly have your hand raised saying “Send me Lord, send me!”
What does it take to go internationally?
Flexibility, agenda-free thinking, funding, immunizations, peanut butter, and “just in case” medicines make international outreach travel all that you imagine and then some.
- Flexibility, or maybe it should be FLEXIBILTY - It is so important to remain in that mode. You will find it key to surviving. Every country runs on its own time, schedule, and expectations. A willingness to adjust is essential.
- Agenda-free, I can do that…or can I? - You may want to encourage that patients see the ultrasound screen; you may want to write on the printed image; and you may think you are there to share all you can. Feel free to change that thinking. For one thing, they may not have all the equipment you are used to having. God brought you there to learn. Listen to Him.
- Funding? I have the money to buy my ticket, but I’ll not ask anyone else - What?! And rob them of the opportunity to share in His work? Remember you are the vessel, but He can bless many as you go and then share what He’s doing.
- Immunizations are just part of it - Bugs, climates, diseases, many new things to ward off as a traveler - this is easy to check and get educated on.
- Peanut butter goes a long way - It is one of God’s basic food groups. Some on a spoon, a dried banana chip, or on a piece of bread; peanut butter is a great source of nutrition.
- “Just in case medicines” are a must have! - A bee sting, a bug bite, a stomach upset, a cut, etc. Be prepared, all kinds of things can happen!
Who’s qualified to go?
Those He’s called.
Hope Imaging recommends taking a team; two registered sonographers, one prayer partner, and one intern. The registered sonographers can rotate with the training and translation. The prayer partner is one who can be trusted with difficult situations – team members, participants, safety, health, technical translations, clinic needs, medical needs…the prayer needs can be endless.
An intern, as defined by Hope Imaging, is one of the following:
- the medical professional trained in limited sonography,
- the medical student interested in missions, or
- the sonography student getting ready to join the work force.
Any of these members can be combined. For example, a registered nurse/sonographer might also serve as prayer partner, or a registered sonographer may be prayer warrior. You get the idea; it’s that flexible thing again!
Who do we teach internationally?
The simple answer is primarily physicians. Physicians are quick learners so keep that in mind as you walk them through the steps to a good image. Be patient and work with them. Remember, they want to learn. That machine has been sitting idle for too long. Let’s get it in use!
The reality is, however, that we teach everyone we cross paths with.
I hope the idea of considering an international, life-affirming imaging trip is of interest to you. For more information, please contact Kama Tate Gregory, CEO, Hope Imaging at This email address is being protected from spambots. You need JavaScript enabled to view it. and/or visit HopeImaging.org to discover where the team is headed next and find out how you might serve.
Our teams need people with a heart for international missions, who are flexible, and who are willing to raise their hand and say, “Send me Lord, send me!”
Connie Ambrecht serves as International Team Coordinator as well as Team Leader for Hope Imaging. She and her husband have been involved with Hope Imaging since its birth in 2005.
